
Optimizing Chronic Care Management Programs for Maximum Benefit
Part 1 of a 3-part series by Rebecca Russell, RemetricHealth
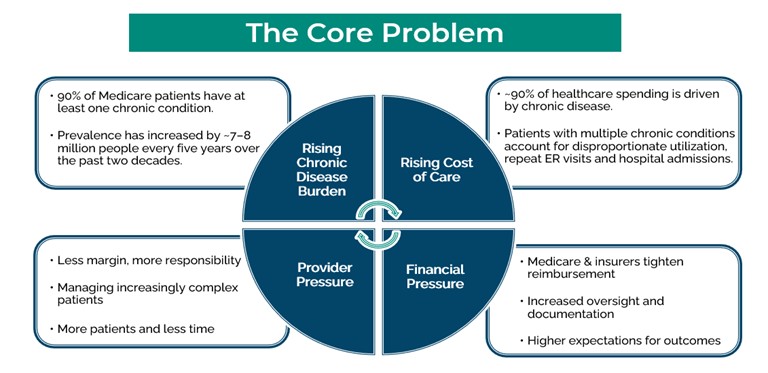
The Growing Burden of Chronic Disease in the U.S.
Chronic diseases have become the norm. Over the past two decades, the U.S. has seen an additional 7–8 million people living with chronic conditions. Currently, 42% of the US population has 2 or more chronic conditions. While 90% of patients in the US who are 65 and older have at least one chronic disease, 64% have two or more.1
These patients often require ongoing care beyond what can be addressed during an office visit alone. Medication management, referrals, monitoring, follow-up, care coordination, and patient engagement are all essential components of managing chronic illness. Much of this work must occur outside of the visit.
Why Office Visits Alone Are No Longer Enough
Historically, healthcare delivery was designed around the office visit. Reimbursement structures, workflows, and clinical documentation were all centered on in-person encounters. As the prevalence of chronic disease has increased, the number of providers per patient has declined, medication adherence for these patients is now at 50%2 and the average no-show rate is 15%3 – additional pressure is added to the office visit.
Managing these patients drives the majority of healthcare spending. In 2024, total healthcare spending reached $5.3 trillion, with approximately 90% attributable to chronic disease.2 As costs rise, healthcare payers respond with tighter reimbursement and higher expectations around quality and outcomes. This pressure flows directly to providers, who are tasked with managing larger patient panels, increasingly complex patients, and more demanding quality metrics. Without a different approach to bridging the gap between visits and engaging patients in their care, the same challenges repeat themselves, creating a vicious cycle.
Fortunately, advances in technology and care management programs have emerged to support providers and close the gap between visits.
The Role of Care Management Programs Between Visits
Medicare and payors are increasingly looking to care management programs to address this gap. Providers are seeking ways to stabilize revenue and improve patient management without adding additional strain to already overextended clinical teams. When implemented correctly—emphasis correctly—care management programs can provide a better way to manage patients, improve outcomes, increase engagement, and generate predictable revenue.
The Evolution of CMS Support for Care Management
Despite the approach of United Healthcare, who has now retracted their position, care management programs are not going away. In fact, they have continued to expand and evolve since the introduction in 2013. CMS has demonstrated a sustained commitment to these services, investing in programs over the last decade that strengthen what happens both between and during office visits, while also making visits more informed and more effective.

For more than a decade, physicians, health systems, and care teams have been implementing Chronic Care Management (CCM) and Remote Patient Monitoring (RPM). When implemented correctly, with the proper care team and clinical workflows in place, these programs work. They reduce hospitalizations, emergency department visits, and total cost of care. This is supported by years of real-world implementations and peer-reviewed evidence.4
At its best, care management does not feel like a program at all—it feels like an extension of the practice. It supports providers, strengthens care teams, and meets patients where they are.
What Comes Next in This Series
In our next installment, we’ll provide an overview of each program, how they differ and how to manage a patient population across programs.
- Medicare Statistics (2025)
- Study reviews medication adherence interventions – Vanderbilt Health
- Lead time for appointment and the no-show rate in an ophthalmology clinic – PMC
- Chronic Conditions among Medicare Beneficiaries:
Association of Remote Patient Monitoring with Mortality and Healthcare Utilization in Hypertensive Patients: a Medicare Claims-Based Study – PubMed & Remote patient monitoring in heart failure: A comprehensive meta‐analysis of effective programme components for hospitalization and mortality reduction – De Lathauwer – 2025 – European Journal of Heart Failure – Wiley Online Library
Leave A Comment