Optimizing Chronic Care Management Programs for Maximum Benefit: A Plain Language Guide to Chronic Care Programs
Today, 42% of the US population has 2 or more chronic conditions. That number is even higher among seniors. Patients with chronic diseases often require ongoing care, well beyond what can be addressed during an office visit alone. Medication management, referrals, monitoring, follow-up, care coordination, and patient engagement are all essential components of managing chronic illness. Much of this work must occur outside of the visit. Technology has advanced, and a number of care management programs have emerged to support providers and close the gap between visits. Chronic Care Management (CCM), Advanced Primary Care Management (APCM), Remote Patient Monitoring (RPM), and Remote Therapeutic Monitoring (RTM) each serve a different purpose, and together they can create a stronger, more sustainable model for supporting patients between visits. The key is not simply adding more services. It is understanding how each program fits into your workflow, your patient population, and your long-term care strategy.
Practices can optimize chronic care management by using the right mix of CCM, APCM, RPM, and RTM based on patient needs, clinical workflows, documentation requirements, and reimbursement opportunities.

What Is Chronic Care Management (CCM)?
Chronic Care Management is designed for patients with two or more chronic conditions and provides a comprehensive care plan specific to a patient’s conditions and requires monthly review with the patient. This includes reviewing the patient’s conditions, medications or changes, symptoms, specialist visits, and overall care coordination. When a patient presents for an office visit, the care plan gives the provider and care team the most up-to-date information at their fingertips. CCM has been in place for years and consists of two primary codes, both of which saw reimbursement increases this year.

What Is Advanced Primary Care Management (APCM)?
Advanced Primary Care Management was introduced in 2025 to address many of the administrative challenges that made older care management models harder to sustain.
It eliminates rigid time counting and is designed to reduce documentation burden. APCM functions as an umbrella model, incorporating elements of CCM, PCM, complex chronic care management, and transitional care management. It is designed to provide what the patient needs in a given month rather than requiring the same activities every month. RPM and RTM are not included within APCM but can be billed in combination with it.
APCM includes ten core service requirements, but these should not be viewed as a checklist. The services must be available to enrolled patients, but only those services that are clinically necessary need to be delivered in a given month. There are no minimum activity thresholds; however, practices must document what was provided to the patient during that month.
- Patient consent needs to be documented in the EHR
- Initiating visit is required for new patients unless seen recently (within 3 years) or received other care management services (within 1 year).
- 24/7 access to their provider or other member of the care team with real-time access to the patient’s medical information to address urgent needs
- Comprehensive care management is similar to CCM but does not require you to go through a detailed care plan each month. You are managing the whole patient but based on what the patient needs. It may be a needs assessment, medication management and reconciliation or oversight of self-management.
- Quality and performance measurement and reporting requires you to assess quality, cost and meaningful use in one of two ways: report the Value in Primary Care MIPS Value Pathway or Participate in a Medicare Shared Savings Accountable Care Organization or similar program.
- Electronic Comprehensive Care Plan does not require a certain template but it must be document in the EHR and available to individuals involved in the patient’s care, including the patient and any care giver. You must be able to routinely access and update the plan.
- Coordinated Care transitions is about staying involved with the patient as they move between providers – referrals, follow-up from emergency visit or hospital stay. This includes a timely follow-up communication within 7 days of discharge.
- Home and Community Care does not mean you are doing a home visit. It means connecting patients to community resources for things like transportation or nutrition. You must support the patient at home by addressing barriers with ongoing coordinating communication and documentation of their strengths, deficits, goals, preferences with other care providers like hospitals and SNFs.
- Patient Population Level Management is proactive identification of care gaps through the analysis of your patient population to identify patients who may need care before they call you and target services to patient in need. This is about reaching out to patients with that proactive care.
- Enhanced Communication means that patients can reach out to you between visits through messaging or email and through a patient portal.
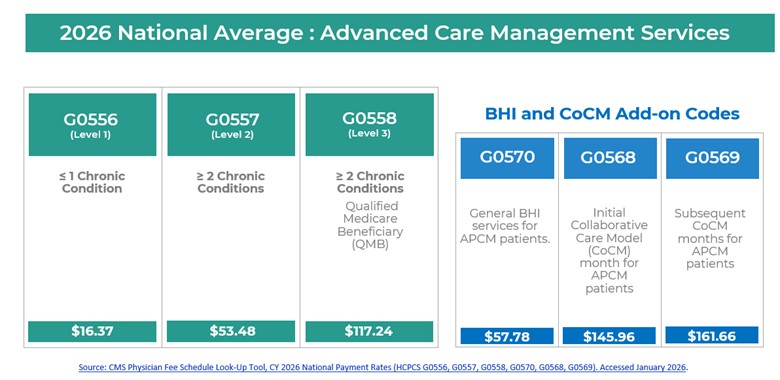
APCM patients are categorized into three levels based on the number of chronic conditions. While Levels 1 and 2 may involve patient cost sharing, Level 3 patients who are Qualified Medicare Beneficiaries do not have a copay. In 2026, CMS added behavioral health and Collaborative Care Management add-on codes.
For example, if an APCM patient has mild depression and receives a depression screening, the behavioral health add-on code G0570 may be billed. Collaborative Care Management, which is more intensive and intended for patients with higher acuity behavioral health needs, requires psychiatric involvement and formal case review to be billable.
For practices currently operating CCM programs, a common question is whether patients should be transitioned to APCM and how to determine which program is appropriate for which patient.
In many cases, both programs can coexist. For example, if a patient has a scheduled CCM interaction and the care team spends 40 minutes in a detailed discussion, CCM may be more appropriate for that month due to higher reimbursement. However, if contact with the patient is brief—such as a short medication request or identification of overdue labs—CCM may not be billable, whereas APCM would be. As long as patients are consented and informed upfront, CCM and APCM can be used together, allowing practices to match the right program to the right patient and situation.
How Remote Patient Monitoring Strengthens Chronic Care Management Programs
Remote Patient Monitoring plays a critical role for patients who benefit from ongoing physiologic data collection outside of the clinical setting. RPM allows providers to supply patients with connected devices that capture and transmit data such as blood pressure, glucose levels, weight, or oxygen saturation. These data are reviewed by the clinical team, enabling early identification of concerning trends and timely intervention before issues escalate into urgent visits or hospitalizations.
The clinical impact of RPM services is well established. Many studies have demonstrated meaningful improvements in disease control and reductions in acute care utilization. Hypertensive and diabetic patients enrolled in RPM programs achieve higher control rates, and these improvements are sustained over time as patients remain engaged. In populations with heart failure, RPM combined with proactive care coordination has been shown to dramatically reduce emergency department visits and hospitalizations while significantly increasing patient engagement and communication with the care team.
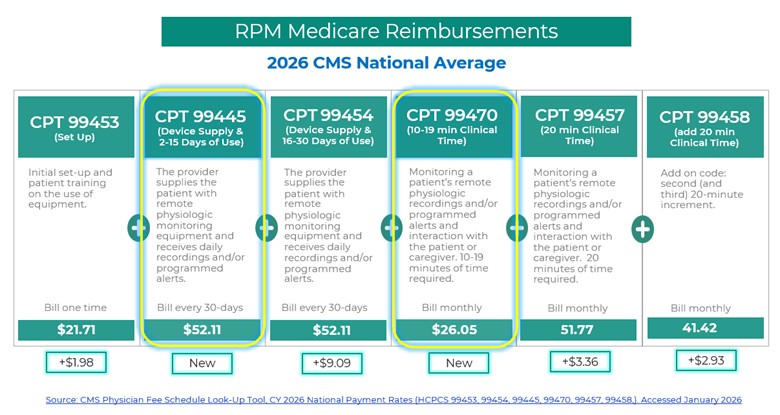
The 2026 Physician Fee Schedule Final Rule brings significant updates that make Remote Patient Monitoring services more flexible, more aligned with real-world clinical workflows, and more financially viable for practices of all sizes. CMS finalized two new RPM CPT codes for 2026 that expand how practices can bill for remote care. These are CPT 99445, which covers device supply and data recording or alert transmission for 2 to 15 days within a 30-day period, and CPT 99470, which covers the first 10 minutes of clinical monitoring time with at least one real-time interactive communication with the patient or caregiver during the calendar month.
Alongside the addition of new RPM CPT codes, CMS also significantly increased reimbursement rates across the existing RPM codes in 2026, reinforcing RPM as a core, sustainable component of longitudinal care rather than a marginal add-on service.
Where Remote Therapeutic Monitoring (RTM) Fits In
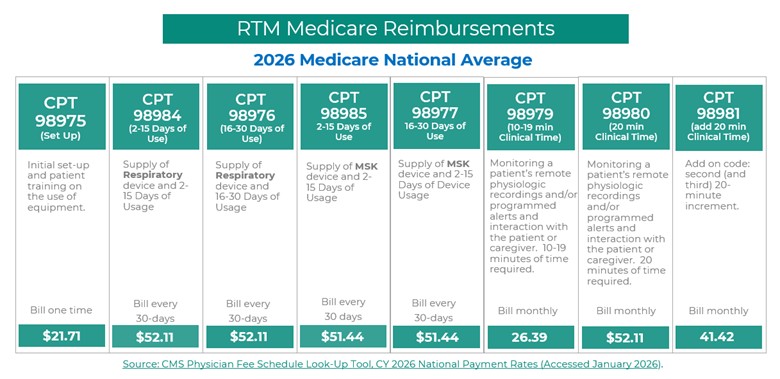
Remote Therapeutic Monitoring has similarly evolved. RTM focuses on non-physiologic data that reflects a patient’s functional status, therapy adherence, or response to treatment, especially in musculoskeletal and rehabilitative care. Like RPM, RTM historically required relatively high thresholds for monitoring duration and clinical time before reimbursement, which limited its use with patients who do not need continuous, high-frequency monitoring. In the 2026 updates, CMS introduced new RTM CPT codes that mirror the philosophy behind the RPM changes by lowering barriers to billing for meaningful care.
By this point, it is likely clear that successful care management requires structure, consistency, and dedicated time. Some practices choose to build internal care teams. Others extend their teams by partnering with a care management organization. Both approaches can be effective when executed well.
When care management is structured intentionally, whether internally or through a partner, it should integrate seamlessly into daily workflows and enhance care delivery without overwhelming clinical teams.
Want to build a more effective care management strategy? RemetricHealth helps practices evaluate where CCM, APCM, RPM, and RTM fit best so they can improve patient support, reduce administrative burden, and strengthen long-term program performance.
What Comes Next in This Series
In our next installment, we’ll cover best practices for structure and implementation of care management programs.
Leave A Comment